Modern lung cancer care relies not only on what a tumor looks like under the microscope, but also on how it behaves at the molecular and immunologic level. One term that appears frequently in pathology and oncology reports is PD-L1. For patients, seeing PD-L1 testing mentioned alongside percentages and scores can be confusing, especially when it is tied directly to treatment recommendations. Understanding what PD-L1 is and how it influences both diagnosis and treatment can help patients make sense of an increasingly complex care landscape.
Understanding PD-L1 in Simple Terms
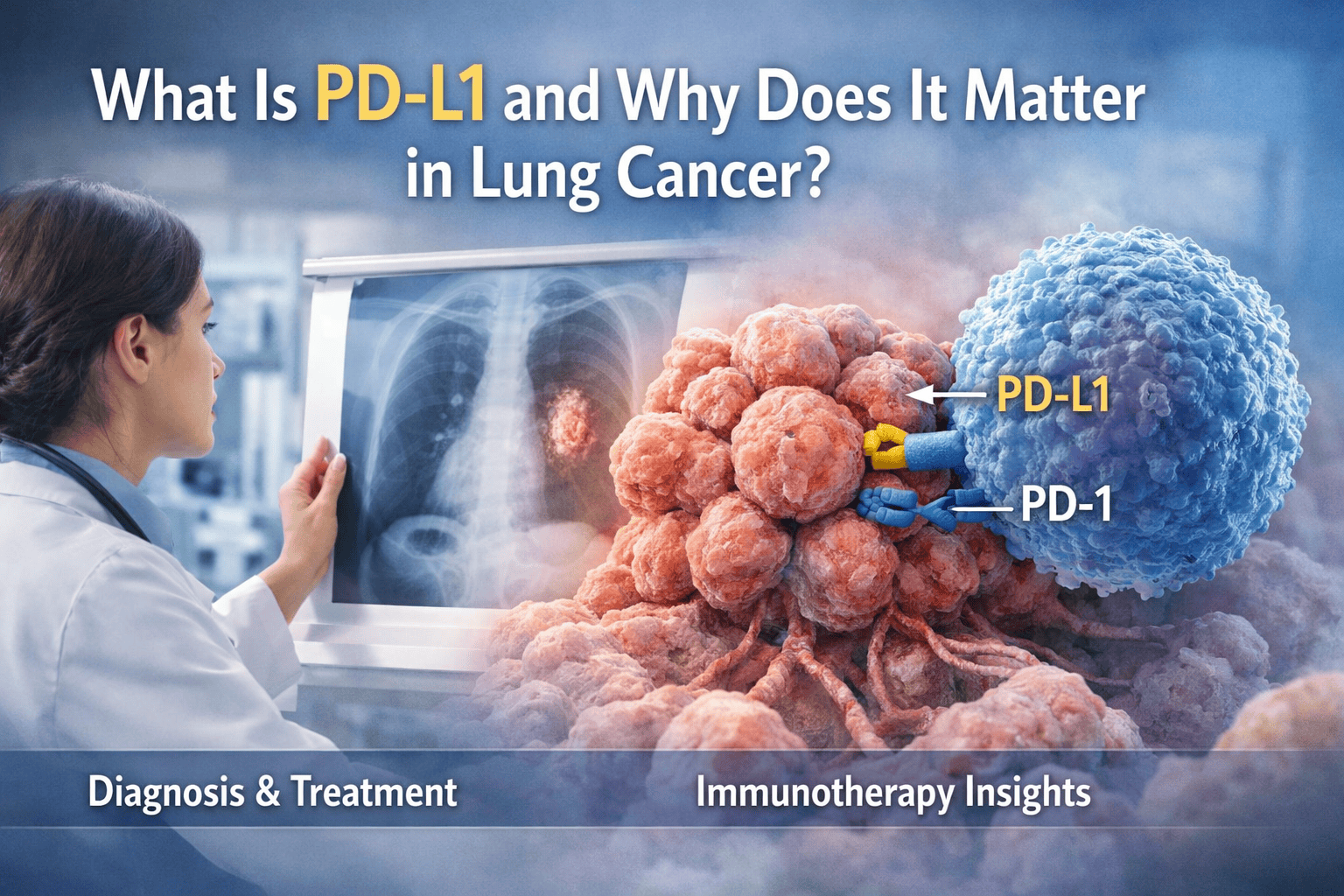
PD-L1 stands for programmed death-ligand 1, a protein that can be expressed on the surface of tumor cells and some immune cells. Its normal role in the body is to help regulate the immune system and prevent excessive immune responses. Cancer cells, however, can exploit PD-L1 as a way to hide from the immune system.
When PD-L1 on tumor cells binds to its partner receptor, PD-1, on immune cells, it sends a signal that dampens the immune response. This allows cancer cells to evade detection and destruction. Recognizing this interaction led to the development of immunotherapies that block the PD-1/PD-L1 pathway.
How PD-L1 Is Tested in Pathology
PD-L1 testing is performed using immunohistochemistry on tumor tissue. A special stain highlights PD-L1 expression, allowing pathologists to estimate how much of the tumor expresses this protein. The result is usually reported as a percentage or score rather than a simple positive or negative.
In lung cancer, PD-L1 testing is most commonly performed in non–small cell lung cancer. It is often ordered at the time of initial diagnosis or when planning systemic therapy. Because PD-L1 testing uses tissue, adequate biopsy samples and careful tissue handling are essential.
The Role of PD-L1 in Diagnosis
PD-L1 is not a diagnostic marker in the traditional sense. It does not determine whether a tumor is cancer, what type of cancer it is, or where it originated. Instead, PD-L1 testing is considered a predictive biomarker, meaning it helps predict how likely a tumor is to respond to certain treatments.
That said, PD-L1 testing has become part of the standard diagnostic workup for many lung cancers because of its direct impact on treatment planning. Its inclusion in the pathology report reflects how closely diagnosis and therapy are now intertwined.
PD-L1 and Immunotherapy
The primary reason PD-L1 testing matters is its role in guiding immunotherapy. Drugs known as immune checkpoint inhibitors target the PD-1/PD-L1 pathway, allowing the immune system to better recognize and attack cancer cells.
In non–small cell lung cancer, higher PD-L1 expression is often associated with a greater likelihood of response to these drugs. In some cases, patients with high PD-L1 expression may be eligible for immunotherapy as a first-line treatment, sometimes without chemotherapy.
Lower or absent PD-L1 expression does not mean immunotherapy will not work, but it may influence how immunotherapy is combined with other treatments or whether it is used later in the treatment course.
How PD-L1 Results Are Reported
PD-L1 results are commonly reported as a tumor proportion score, which reflects the percentage of tumor cells showing PD-L1 staining. Different treatment approvals and clinical guidelines use specific cutoff values to guide therapy decisions.
Because of this, accurate interpretation and reporting are critical. Small differences in scoring can influence treatment eligibility, making quality pathology and experience especially important.
Limitations of PD-L1 Testing
While PD-L1 is an important biomarker, it is not perfect. PD-L1 expression can vary within different areas of the same tumor and can change over time, especially after treatment. Small biopsies may not fully capture this variability.
Technical factors, such as the specific antibody used or tissue preservation, can also affect results. Additionally, some patients with low or negative PD-L1 expression still respond well to immunotherapy, while some with high expression may not.
For these reasons, PD-L1 is one piece of a larger decision-making framework rather than a standalone answer.
PD-L1 in Combination With Other Biomarkers
In lung cancer, PD-L1 testing is often considered alongside molecular testing for genetic alterations and other clinical factors. Tumors with certain mutations may be treated differently, even if PD-L1 expression is high.
This integrated approach highlights the evolving role of pathology, which now bridges diagnosis, prognosis, and treatment selection in a single report.
Why Expert Pathology Review Matters for PD-L1
Interpreting PD-L1 staining requires training and experience. Determining which cells should be counted, recognizing true staining versus background, and applying scoring criteria correctly are all essential for reliable results.
Expert pathology review can be especially valuable when treatment decisions hinge on PD-L1 levels, when tissue is limited, or when results seem inconsistent with the clinical picture.
What Patients Can Ask About PD-L1
Patients who see PD-L1 results on their pathology report can ask their care team how the score was determined, what it means for treatment options, and how it fits with other test results. Understanding the role of PD-L1 can make treatment discussions feel more transparent and less overwhelming.
Bringing Meaning to a Complex Marker
PD-L1 represents a shift in how cancer is understood and treated, moving beyond traditional classifications toward immune-based therapy. While the testing and terminology can feel complex, its purpose is to personalize treatment and improve outcomes.
For patients seeking clarity about PD-L1 testing and how it affects their diagnosis and treatment, Honest Pathology provides independent expert pathology review with clear, patient-centered explanations. Their focus is on helping patients understand not just what their results are, but what those results truly mean for their care and next steps.