Intestinal metaplasia on gastroesophageal biopsy is a common yet often alarming finding that leaves many patients searching online for straightforward answers about its significance, causes, and long-term outlook. When pathologists identify intestinal-type cells in tissue samples taken from the lower esophagus or gastroesophageal junction during an upper endoscopy, it signals that the normal lining has undergone a change in response to chronic irritation. This finding does not mean cancer is present, but it represents a precancerous shift that warrants attention and monitoring in many cases.
Understanding exactly what intestinal metaplasia means in the context of gastroesophageal biopsies can ease anxiety and help patients become active participants in their care. Honest Pathology provides expert pathology consultations that break down these reports into clear, accessible language, empowering individuals with the precise insights needed to discuss management options confidently with their gastroenterologist.
What Is Intestinal Metaplasia on Gastroesophageal Biopsies?
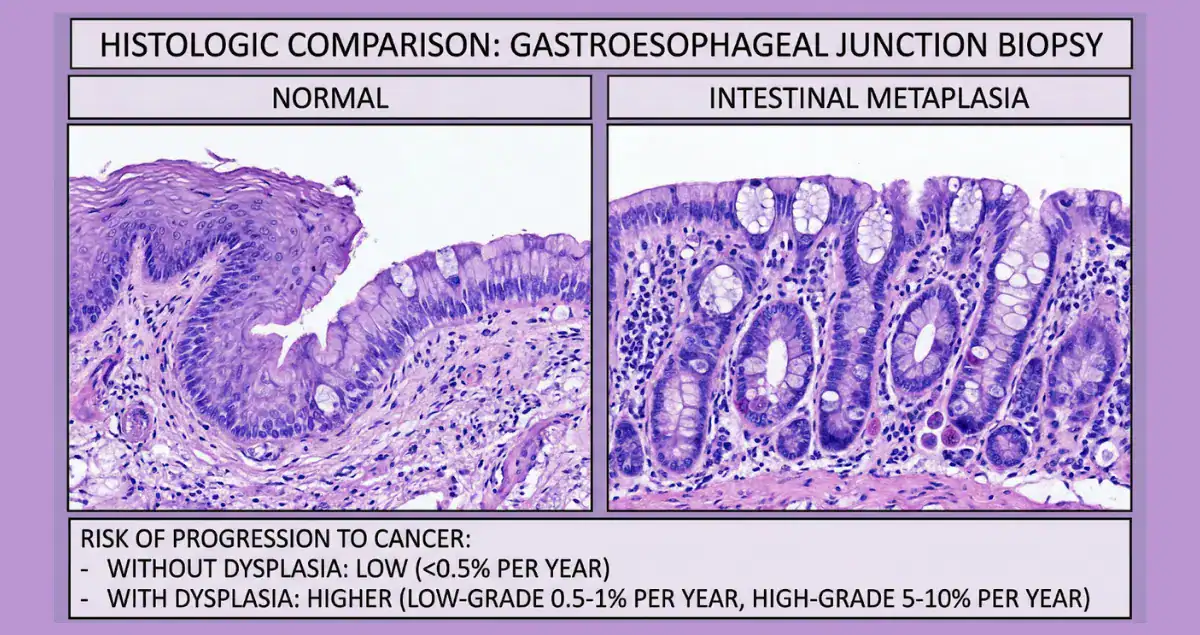
Intestinal metaplasia occurs when the normal squamous cells lining the esophagus or the junction with the stomach are replaced by cells that resemble those found in the intestines, complete with goblet cells that produce mucus. In gastroesophageal biopsies, this change is most often discovered incidentally during evaluation for heartburn, reflux symptoms, or routine screening. When the metaplasia involves the tubular esophagus above the gastroesophageal junction, it defines Barrett’s esophagus, the classic precancerous condition linked to chronic gastroesophageal reflux disease.
Biopsies taken precisely at or just below the junction may instead show intestinal metaplasia of the gastroesophageal junction, sometimes called cardia intestinal metaplasia. Pathologists look for specific histologic features, such as the presence of goblet cells confirmed by special stains like Alcian blue, to make the diagnosis. Patients frequently encounter terms like “specialized intestinal metaplasia” or “Barrett’s mucosa” in their reports, and expert review helps clarify whether the finding represents true esophageal involvement or a junctional change, which can influence follow-up recommendations.
Causes and Risk Factors for Intestinal Metaplasia in the Gastroesophageal Region
The primary driver of intestinal metaplasia in gastroesophageal biopsies is long-standing exposure to stomach acid and bile through gastroesophageal reflux. Repeated injury to the delicate esophageal lining prompts the tissue to adapt by adopting a more acid-resistant intestinal-type lining. Obesity, particularly central abdominal fat, increases intra-abdominal pressure and promotes reflux, while smoking, alcohol use, and a diet high in processed foods or low in fruits and vegetables can further elevate risk.
Certain genetic factors and family history of esophageal or gastric cancer may also play a role in susceptibility. Helicobacter pylori infection, more commonly associated with gastric intestinal metaplasia elsewhere in the stomach, can occasionally contribute near the junction, though its role is less dominant in pure gastroesophageal findings. Unlike acute damage that heals quickly, the chronic nature of reflux allows these cellular changes to become established over years, which is why patients with longstanding heartburn symptoms are more likely to have this biopsy result. Lifestyle and medical history details shared during pathology consultation help contextualize the finding and highlight modifiable risk factors that could slow progression.
Answering the Most Common Questions About Intestinal Metaplasia on Gastroesophageal Biopsy
Patients newly facing this diagnosis often type the same urgent questions into search engines. Does intestinal metaplasia mean I have Barrett’s esophagus? When confirmed in the esophagus proper, yes, it meets the criteria for Barrett’s esophagus; at the junction alone, guidelines sometimes treat it more conservatively as a lower-risk variant. Is it cancer or will it become cancer? Intestinal metaplasia itself is not cancer and carries no immediate threat, but it is considered a precancerous condition because the altered cells have taken the first step on a pathway that can eventually lead to dysplasia and esophageal adenocarcinoma. Another frequent query concerns symptoms: most people with intestinal metaplasia experience only the underlying reflux symptoms such as heartburn, regurgitation, or difficulty swallowing, while the metaplasia itself produces no unique sensations. Patients also ask about the need for immediate treatment or lifestyle changes.
While no single pill reverses the metaplasia, daily proton pump inhibitors to control acid, weight loss, elevating the head of the bed, and avoiding trigger foods can reduce ongoing injury and may stabilize or even partially regress the changes in some cases. Genetic testing is rarely indicated unless there is a strong family history, and the biopsy itself does not cause the metaplasia but simply reveals it. Honest Pathology consultations directly address these questions by reviewing the exact wording of the report, explaining the location and extent of the metaplasia, and connecting the microscopic details to each patient’s clinical picture.
Prognosis and Risk of Progression to Cancer
The prognosis for patients with intestinal metaplasia on gastroesophageal biopsy is generally favorable, particularly when no dysplasia is present. For nondysplastic Barrett’s esophagus, the annual risk of progressing to esophageal adenocarcinoma is approximately 0.3 to 0.5 percent, meaning the vast majority of individuals never develop cancer. Short-segment disease, defined as less than three centimeters of involved esophagus, carries an even lower risk, and recent 2025 guidelines from the American Gastroenterological Association suggest against routine surveillance endoscopy for columnar-lined esophagus measuring less than one centimeter with intestinal metaplasia due to the minimal progression potential.
Factors that worsen prognosis include longer segments of metaplasia, male sex, older age, smoking history, and the presence of low-grade or high-grade dysplasia on biopsy. When dysplasia is absent, the ten-year cumulative risk of cancer remains under two percent for most patients, and regular surveillance combined with acid control can detect any early changes while they remain highly treatable. Patients often search for survival statistics, and the key takeaway is that early identification of intestinal metaplasia allows intervention long before cancer develops, with five-year survival rates for early-stage esophageal adenocarcinoma exceeding ninety percent when caught through monitoring programs. Pathology consultation plays a pivotal role here by confirming the absence or presence of dysplasia and assessing any additional molecular or histologic features that refine individual risk estimates.
Treatment and Management Options for Intestinal Metaplasia
Management of intestinal metaplasia on gastroesophageal biopsies centers on controlling reflux and performing periodic surveillance rather than immediate eradication in most nondysplastic cases. Proton pump inhibitors remain the cornerstone of therapy, often prescribed at higher doses to heal inflammation and minimize further cellular stress. Endoscopic surveillance intervals depend on the extent of metaplasia and dysplasia status: every three to five years for nondysplastic long-segment Barrett’s esophagus, with shorter or no routine follow-up for very short segments per current guidelines. If low-grade dysplasia is identified, more frequent examinations or endoscopic eradication therapies such as radiofrequency ablation may be discussed.
Advanced cases with high-grade dysplasia or early cancer shift toward endoscopic resection combined with ablation. Lifestyle modifications, including weight management, smoking cessation, and dietary adjustments, complement medical therapy and improve overall prognosis. Patients frequently wonder whether surgery such as fundoplication is necessary; it is usually reserved for those with refractory reflux symptoms despite optimal medication. Clinical trials exploring chemoprevention or advanced imaging techniques continue to evolve, offering additional options for those at higher risk. Expert pathology review ensures that the biopsy findings align with the most up-to-date management protocols, preventing both over-treatment of low-risk cases and under-surveillance of those who need closer attention.
How Pathology Consultations Empower Patients Facing Intestinal Metaplasia
Receiving a pathology report that mentions intestinal metaplasia can feel overwhelming when the language is dense with medical terminology and the implications seem uncertain. Honest Pathology offers specialized pathology consultations tailored to gastroesophageal biopsy findings, providing patients with a clear, personalized explanation of the report’s details, the exact location and extent of the metaplasia, and any subtle features that influence risk or management. Rather than leaving individuals to interpret conflicting online information alone, these consultations translate technical histology into practical next steps, such as recommended surveillance timing or questions to ask the gastroenterologist. Patients emerge better equipped to weigh treatment choices, understand their personal prognosis, and advocate for care that matches their values and risk profile. In a condition where precise classification can shift recommendations dramatically, this level of clarity transforms anxiety into informed confidence.
Intestinal metaplasia on gastroesophageal biopsy represents a detectable and manageable step on the pathway from chronic reflux to potential cancer, yet for the great majority of patients it remains a stable finding that never progresses further. By seeking expert pathology consultation early, individuals gain the knowledge needed to navigate surveillance, lifestyle adjustments, and medical therapies with clarity and partnership. Honest Pathology exists to deliver exactly that understanding, ensuring every patient can approach their diagnosis with accurate information, reduced worry, and a proactive plan for long-term health.