When a melanoma is diagnosed, one of the most important numbers in the pathology report is the Breslow depth. This measurement plays a central role in determining melanoma stage, estimating prognosis, guiding surgical management, and deciding whether additional procedures such as sentinel lymph node biopsy are needed.
Because Breslow depth directly influences treatment decisions, it is one of the most frequently reviewed and searched terms in melanoma pathology. At Honest Pathology, we regularly help patients interpret this measurement and understand what it means in the broader context of their diagnosis.
What Is Breslow Depth?
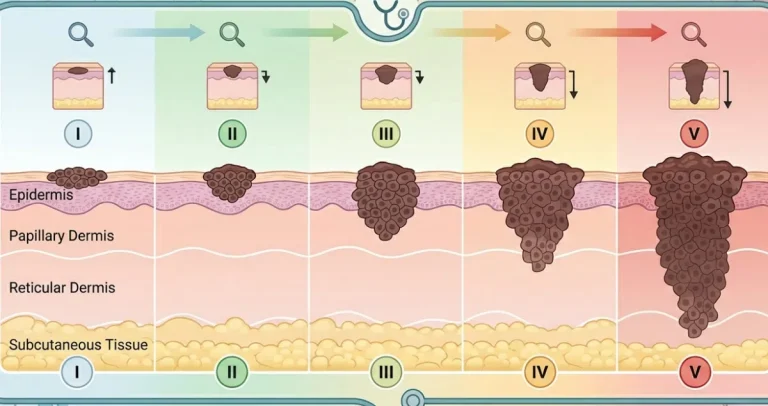
Breslow depth is the measurement of how deeply a melanoma has penetrated into the skin. It is recorded in millimeters and represents the vertical thickness of the tumor.
The pathologist measures Breslow depth from the top of the epidermis, or from the base of any ulceration if the surface layer is missing, down to the deepest point of tumor invasion. This measurement reflects how far the melanoma cells have grown beneath the surface.
Unlike diameter, which describes how wide a lesion appears, Breslow depth measures how deep it extends. Depth, rather than width, is the most important factor in predicting behavior.
Why Breslow Depth Is So Important
Breslow depth is the single most powerful predictor of outcome in localized melanoma. As melanoma grows deeper into the skin, the risk of spread to lymph nodes or distant organs increases.
Melanomas are staged using the TNM system, and tumor thickness is central to the “T” category. Small differences in depth can change the stage classification and influence treatment recommendations.
Thin melanomas generally carry an excellent prognosis. Thicker melanomas require more extensive surgical margins and may prompt consideration of lymph node evaluation or additional therapy.
How Breslow Depth Is Measured
After the lesion is removed, the specimen is processed in the pathology laboratory. The tissue is embedded in paraffin, sliced into thin sections, stained, and examined under a microscope.
Using a calibrated eyepiece or digital measurement system, the pathologist identifies the top of the epidermis and measures vertically to the deepest melanoma cell. The measurement is recorded in millimeters to the nearest tenth or hundredth.
If the melanoma is ulcerated, the measurement begins at the base of the ulcer rather than the missing surface. This ensures consistent staging.
In rare cases, a superficial shave biopsy may not capture the full depth of the tumor. If the base of the lesion is transected, the reported Breslow depth may represent a minimum estimate. This is one reason why complete excision is often recommended after an initial biopsy diagnosis.
 What Different Breslow Depth Ranges Mean
What Different Breslow Depth Ranges Mean
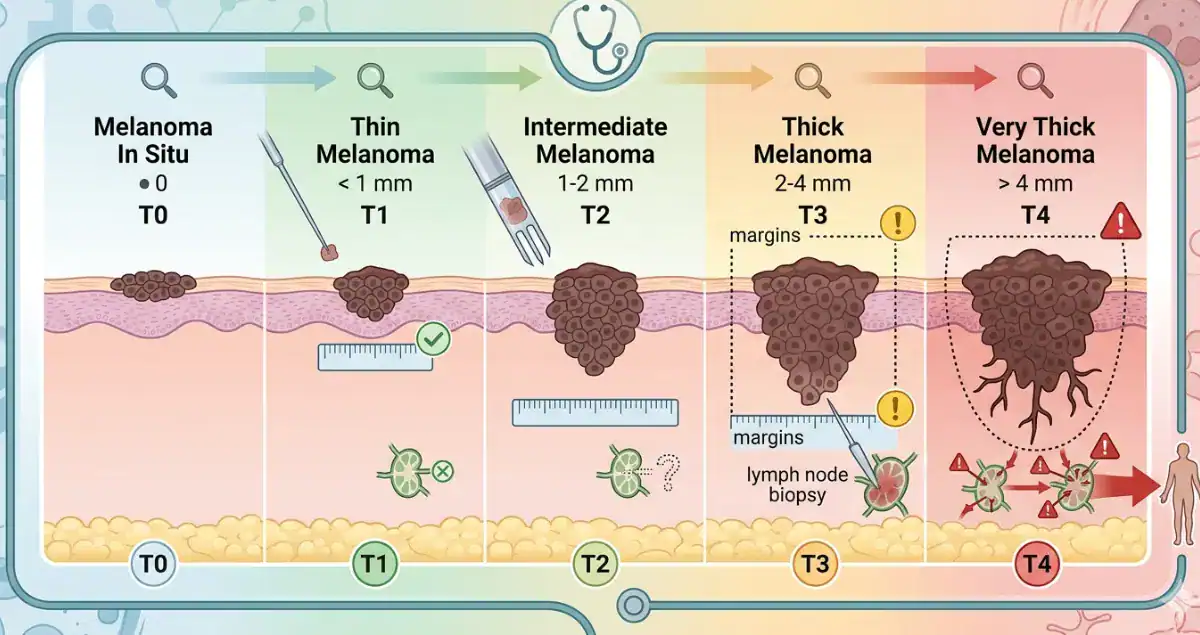
Melanomas are broadly categorized by thickness.
Thin melanomas measure 1.0 millimeter or less. These are often stage T1 lesions and generally have a very favorable prognosis, especially if there is no ulceration.
Intermediate-thickness melanomas measure between 1.01 and 4.0 millimeters. These lesions carry a higher risk of lymph node involvement, and sentinel lymph node biopsy is often considered.
Thick melanomas measure greater than 4.0 millimeters. These have a higher risk of regional and distant spread and may require more extensive staging and systemic evaluation.
Even small differences, such as 0.8 millimeters versus 1.1 millimeters, can influence recommendations for additional procedures.
Does a Higher Breslow Depth Mean Worse Prognosis?
In general, increasing Breslow depth correlates with higher risk. However, it is not the only factor that determines outcome.
Ulceration, mitotic rate, lymphovascular invasion, and sentinel lymph node status also influence prognosis. A thin melanoma with ulceration may behave more aggressively than a slightly thicker lesion without high-risk features.
Still, Breslow depth remains the cornerstone measurement in early-stage melanoma.
It is important to remember that many melanomas are detected at thin stages, particularly when skin checks and biopsies are performed promptly. Early detection significantly improves outcomes.
What Is the Relationship Between Breslow Depth and Sentinel Lymph Node Biopsy?
One of the most common treatment decisions influenced by Breslow depth is whether to perform a sentinel lymph node biopsy.
For melanomas less than 0.8 millimeters without ulceration, sentinel lymph node biopsy is generally not recommended because the risk of nodal spread is very low.
For melanomas 0.8 millimeters or thicker, or thinner melanomas with ulceration, sentinel lymph node biopsy is often discussed. As thickness increases, the likelihood of microscopic lymph node involvement rises.
This procedure helps determine whether cancer cells have spread beyond the primary tumor site and provides important staging information.
Can Breslow Depth Change After Re-Excision?
Sometimes a melanoma is initially diagnosed on a partial biopsy. If the base of the lesion was not fully sampled, the initial Breslow depth may underestimate the true thickness.
After a complete excision, additional deeper sections may reveal a greater depth than originally reported. In such cases, staging and management recommendations may be adjusted accordingly.
This does not mean the melanoma grew rapidly in the interim. Rather, it reflects more complete sampling of the tumor.
At Honest Pathology, we emphasize the importance of understanding whether a biopsy fully captured the lesion when interpreting Breslow depth measurements.
How Accurate Is Breslow Depth?
When measured on a properly excised and fully sampled lesion, Breslow depth is highly reproducible and reliable. It is a standardized measurement used worldwide and incorporated into international melanoma staging guidelines.
Pathologists are trained to measure depth precisely because small differences can influence staging thresholds.
Occasionally, technical factors such as tissue orientation or prior partial biopsy can complicate measurement, but these issues are typically addressed in the pathology report.
What Breslow Depth Does Not Tell You
Although Breslow depth is critically important, it does not provide a complete picture of metastatic risk on its own.
It does not determine whether cancer has already spread to distant organs. Imaging and lymph node evaluation address those questions.
It also does not predict response to immunotherapy or targeted therapy. Molecular testing and genetic features may guide those decisions in advanced disease.
Breslow depth is most powerful in early-stage melanoma and is primarily a tool for staging and surgical planning.
The Bottom Line on Breslow Depth
Breslow depth is the measurement of how deeply a melanoma penetrates into the skin, expressed in millimeters. It is the most important factor in determining tumor stage and one of the strongest predictors of prognosis in localized melanoma.
Thinner melanomas generally have an excellent outlook and may require only surgical excision with appropriate margins. Thicker melanomas may prompt sentinel lymph node biopsy and closer follow-up.
If a pathology report lists Breslow depth, that number is central to understanding the diagnosis. When interpreted alongside ulceration status and other microscopic features, it provides a clear framework for treatment planning.
Clear communication about pathology findings is essential in melanoma care. Understanding Breslow depth transforms a single number on a report into meaningful insight about stage, management, and next steps.