When a melanoma is diagnosed, one of the terms that often appears in a pathology report is Clark level. While Breslow depth is now the primary predictor of melanoma prognosis, Clark level continues to provide important context, particularly for thinner melanomas. Understanding Clark level helps patients and clinicians interpret the extent of tumor invasion, anticipate potential risks, and guide follow-up care.
At Honest Pathology, we work with patients to clarify these measurements and explain what they mean for prognosis and treatment planning.
What Clark Level Measures
Clark level describes the anatomical depth of melanoma invasion in the skin. Unlike Breslow depth, which measures vertical thickness in millimeters, Clark level identifies the deepest layer of skin reached by the tumor.
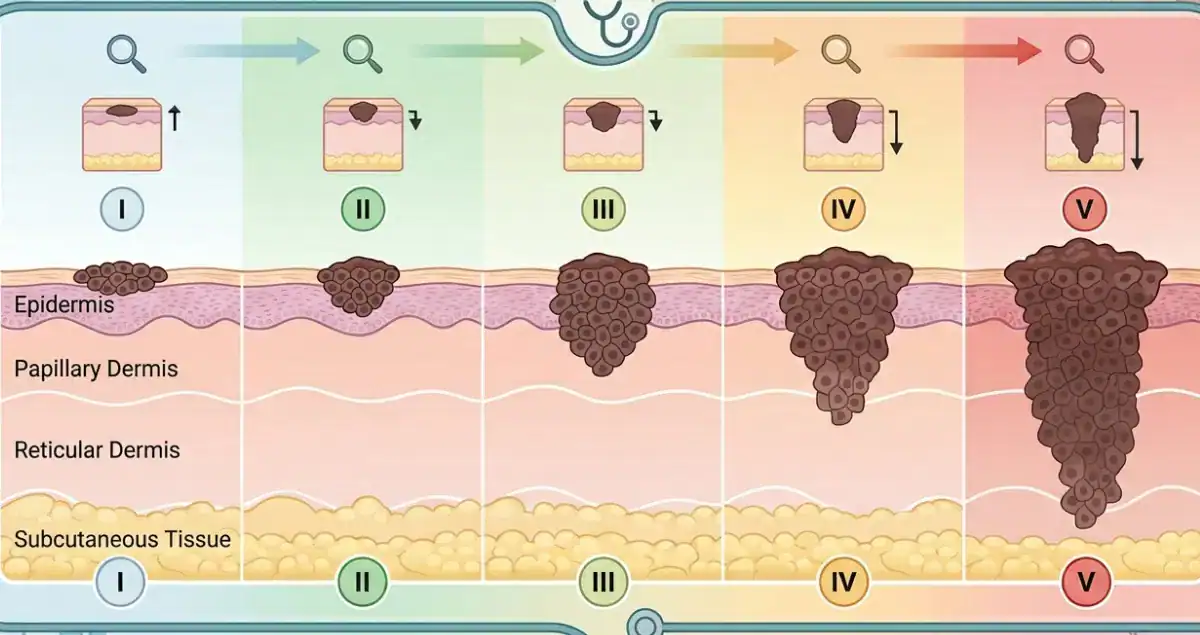
The five Clark levels are:
Level I indicates the melanoma is confined to the epidermis, or the outermost skin layer. This is also known as melanoma in situ, meaning it has not yet penetrated deeper layers.
Level II occurs when the melanoma invades the papillary dermis, the thin upper layer of the dermis just beneath the epidermis.
Level III means the tumor fills and expands the papillary dermis, reaching the junction between the papillary and reticular dermis.
Level IV indicates invasion into the reticular dermis, a deeper dermal layer that provides structural support to the skin.
Level V occurs when melanoma penetrates into the subcutaneous tissue beneath the dermis.
By describing the specific layer of invasion, Clark level provides an anatomical perspective on how far the melanoma has progressed.
Clark Level and Prognosis
Clark level has historically been used to estimate prognosis. In general, the deeper the melanoma penetrates, the higher the risk of metastasis and recurrence.
Melanomas limited to the epidermis (Level I) have an excellent prognosis, with almost no risk of spread. Levels II and III carry a low but measurable risk, particularly if other high-risk features like ulceration are present. Level IV melanomas, which reach the reticular dermis, are associated with a higher likelihood of regional lymph node involvement, while Level V melanomas extending into subcutaneous tissue carry the highest risk of metastasis.
Although Breslow depth is now considered more predictive of outcomes, Clark level remains informative, especially in thin melanomas where precise measurement in millimeters may be very small. For example, a 0.6-millimeter melanoma confined to the papillary dermis (Clark II) generally has a lower risk than a 0.6-millimeter lesion reaching the reticular dermis (Clark IV).
 How Clark Level Is Determined
How Clark Level Is Determined
After a melanoma is excised, the pathology laboratory processes the specimen by embedding it in paraffin, slicing it into thin sections, and staining them for microscopic examination.
The pathologist identifies the epidermis, dermis, and subcutaneous tissue and determines the deepest layer containing melanoma cells. This layer is assigned the Clark level.
Clark level is often reported alongside Breslow depth, ulceration, mitotic rate, and margin status. Together, these features provide a detailed picture of tumor behavior.
Clark Level in Thin Versus Thick Melanomas
Clark level is particularly meaningful for melanomas less than 1 millimeter thick. In these cases, Breslow depth alone may not provide enough context about the risk of nodal spread. A thin melanoma confined to the upper dermis (Clark II) generally carries minimal risk, while one of similar thickness reaching the reticular dermis (Clark IV) may prompt closer follow-up and discussion of sentinel lymph node biopsy.
For thicker melanomas, Breslow depth is the dominant predictor of prognosis, and Clark level adds descriptive detail rather than changing management. Nevertheless, reporting Clark level remains standard practice because it helps pathologists document anatomical invasion clearly.
Clark Level and Surgical Margins
While surgical margins are usually guided by Breslow depth, Clark level can confirm that excision is adequate for the anatomical depth of invasion. Thin melanomas confined to the epidermis may require narrow margins, while deeper melanomas extending into the dermis or subcutaneous tissue require wider excision to ensure complete removal.
Understanding the Clark level helps clinicians plan surgery appropriately and anticipate potential challenges in achieving negative margins.
Clark Level and Sentinel Lymph Node Biopsy
Clark level also influences the decision to perform a sentinel lymph node biopsy, particularly in thin melanomas. Melanomas under 0.8 millimeters without ulceration are usually low risk and may not require lymph node evaluation. If the melanoma is thin but invades deeper dermal layers (Clark III–IV) or shows ulceration, sentinel lymph node biopsy may be considered to check for microscopic spread.
This evaluation helps refine staging and guide treatment planning, even in early melanomas.
Limitations of Clark Level
Clark level is less precise than Breslow depth and can vary between pathologists. The boundaries between dermal layers are sometimes subtle, leading to potential variability in level assignment.
Additionally, Clark level does not quantify vertical thickness, which is why Breslow depth is considered the primary prognostic measure. Clark level alone cannot predict metastasis or recurrence risk with the same accuracy as Breslow depth combined with other features such as ulceration, mitotic rate, and lymph node status.
Clark Level and Pathology Reports
A typical melanoma pathology report may list Clark level alongside Breslow depth, ulceration, mitotic rate, and margins. For example, a report could read: “Superficial spreading melanoma, Breslow depth 0.9 mm, Clark level III, no ulceration, mitotic rate 1/mm², negative margins.”
This provides a clear description of both vertical thickness and anatomical invasion, helping clinicians determine prognosis and next steps in care.
At Honest Pathology, we help patients interpret these reports, explain the significance of Clark level, and understand how it fits into the overall picture of melanoma staging.
What Patients Should Know
Clark level is primarily a descriptive measure of melanoma penetration into the skin. While it is not the most critical prognostic factor for thick melanomas, it is useful for thin lesions and provides context for surgical and follow-up decisions.
Patients should understand that Clark level is reported alongside Breslow depth, ulceration, and other histologic features to provide a comprehensive assessment. A higher Clark level indicates deeper anatomical invasion but must be interpreted in conjunction with other measurements to estimate risk accurately.
The Bottom Line
Clark level is a historical and anatomical tool for describing how deeply melanoma has invaded the skin. It is most relevant for thin melanomas under 1 millimeter in thickness, providing additional information about risk that complements Breslow depth.
By combining Clark level with Breslow depth, ulceration, mitotic rate, and margin status, clinicians can more accurately stage melanoma, guide treatment decisions, and determine appropriate follow-up. At Honest Pathology, we aim to make these concepts understandable and actionable, helping patients feel informed and empowered as they navigate their diagnosis.