When colon cancer is first diagnosed, it is usually identified through a colonoscopy biopsy. For many patients, the initial pathology report provides the first confirmation of cancer. However, an important and often misunderstood reality is that colon cancer can be understaged on biopsy. The stage determined after surgical resection is frequently more complete and sometimes different from what was suspected at the time of biopsy.
Understanding how biopsy and resection specimens differ is essential for interpreting pathology reports and setting expectations about staging, treatment, and prognosis. At Honest Pathology, we regularly help patients and clinicians navigate these distinctions and clarify why the final surgical pathology report carries the most weight in determining stage.
What a Colon Cancer Biopsy Actually Shows
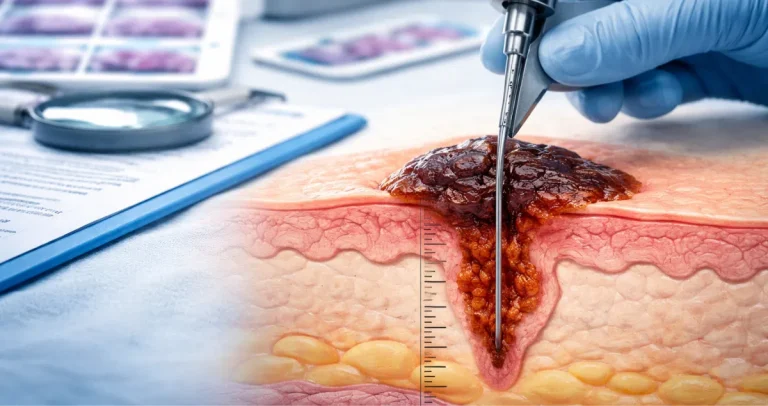
During a colonoscopy, if a suspicious mass or ulcerated lesion is identified, the gastroenterologist takes small tissue samples using biopsy forceps. These samples are typically only a few millimeters in size and include superficial portions of the tumor.
Under the microscope, the pathologist examines these fragments to determine whether cancer is present. A biopsy can confirm adenocarcinoma, identify tumor grade, and sometimes suggest certain molecular features. However, a biopsy cannot fully assess how deeply the tumor invades the colon wall, whether lymph nodes are involved, or whether cancer has spread beyond the colon.
This limitation is central to why colon cancer may appear “early” on biopsy but be assigned a higher stage after surgery.
Why Colon Cancer Can Be Understaged on Biopsy
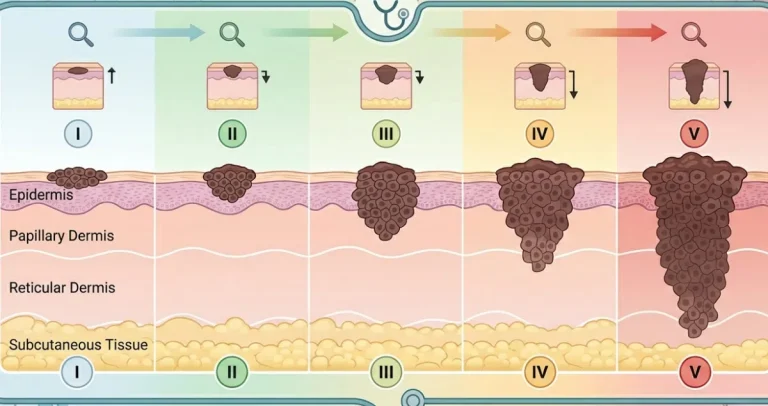
Colon cancer staging depends largely on how deeply the tumor invades through the layers of the colon wall and whether it spreads to lymph nodes or distant organs. A superficial biopsy often samples only the top layers of the tumor.
The colon wall has several layers, including the mucosa, submucosa, muscularis propria, and surrounding fatty tissue. Invasion into deeper layers significantly changes the tumor stage. Because biopsy samples rarely include the full thickness of the colon wall, they cannot reliably determine the depth of invasion.
As a result, a biopsy report may confirm adenocarcinoma but cannot accurately assign a complete pathologic stage. Imaging studies such as CT scans can provide additional clues, but definitive staging requires examination of the entire resected tumor.
Understaging on biopsy does not mean an error occurred. It reflects the inherent limitation of sampling a small portion of a much larger tumor.
How Surgical Resection Provides Complete Staging
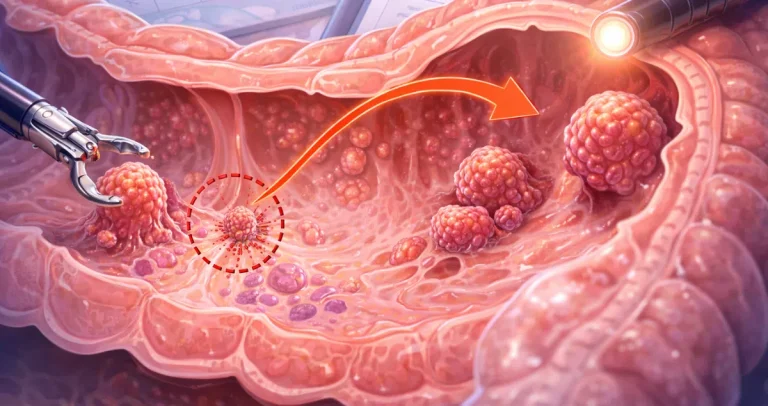
After a colon cancer diagnosis on biopsy, surgery is typically performed to remove the tumor and regional lymph nodes. The surgical specimen allows the pathologist to examine the entire mass, measure its size, and assess how far it penetrates the colon wall.
Most importantly, the resection specimen includes lymph nodes. The presence or absence of cancer in these lymph nodes determines whether the cancer is stage III. Biopsies do not sample lymph nodes, so nodal involvement cannot be assessed at that stage.
The pathologist also evaluates margins, lymphovascular invasion, perineural invasion, and tumor budding. These features are critical for accurate staging and prognosis but cannot usually be assessed on small biopsy fragments.
For these reasons, the final pathologic stage determined after resection is considered definitive.
 Differences Between Biopsy Reports and Resection Reports
Differences Between Biopsy Reports and Resection Reports
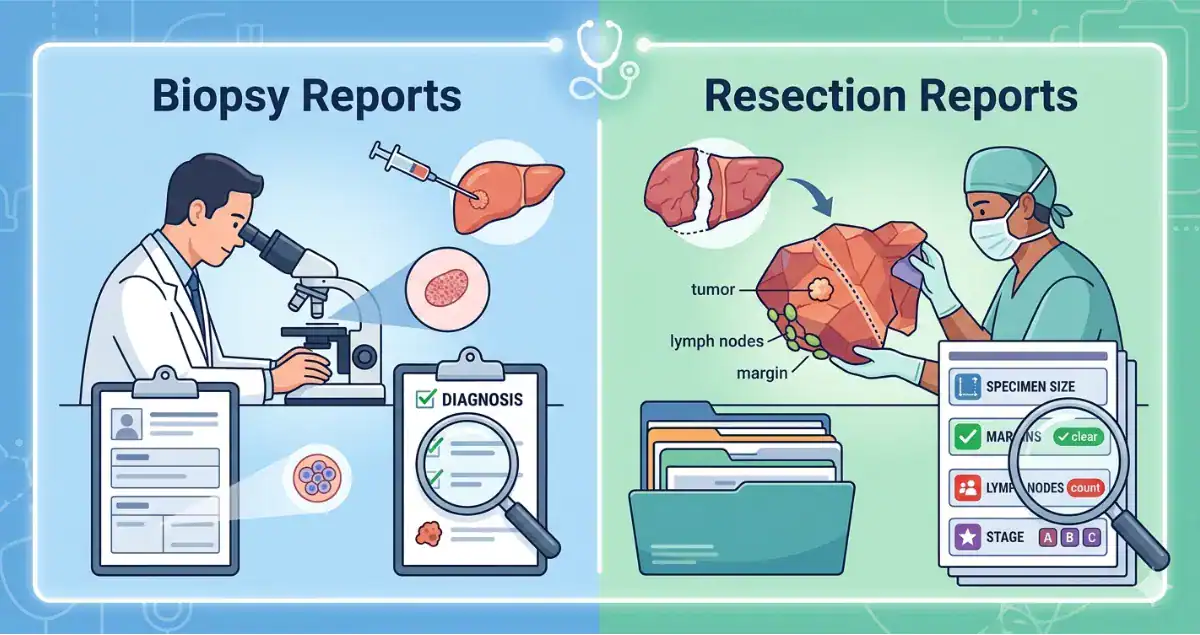
Patients are sometimes surprised when the wording of their final surgical pathology report differs from the initial biopsy. The biopsy report is focused primarily on diagnosis. It answers whether cancer is present and describes the tumor type and grade.
The resection report is far more detailed. It includes tumor size, depth of invasion, lymph node status, margin status, and additional microscopic features. It also assigns a TNM stage, which is the standardized staging system for colon cancer.
It is common for a biopsy to describe “invasive adenocarcinoma” without specifying stage. After surgery, the tumor may be classified as stage I, II, or III depending on the full pathologic findings. Occasionally, imaging may suggest a certain stage preoperatively, but final staging can still differ based on microscopic evaluation.
Can a Biopsy Ever Overstage Colon Cancer?
While understaging is more common, overinterpretation can also occur in rare cases. For example, a biopsy may show high-grade dysplasia or intramucosal carcinoma, which is confined to the mucosa and does not have access to lymphatic channels. In some cases, what appears invasive in a fragmented biopsy may ultimately represent a superficially invasive tumor without deeper spread in the resection specimen.
However, because biopsies are limited samples, they are generally more likely to underestimate tumor depth than overestimate it.
Why Imaging and Biopsy Together Still Do Not Equal Final Stage
Modern colon cancer evaluation often includes CT imaging before surgery. Imaging can estimate tumor size, detect enlarged lymph nodes, and identify distant metastases. Even so, imaging cannot reliably detect microscopic lymph node involvement or subtle invasion into surrounding tissues.
Biopsy confirms the presence of cancer. Imaging provides a macroscopic overview. Only surgical resection allows for microscopic confirmation of tumor depth and nodal spread.
This is why treatment decisions such as chemotherapy are based on final surgical pathology rather than biopsy findings alone.
What It Means If the Stage Changes After Surgery
It can be unsettling to learn that a cancer thought to be early based on biopsy or imaging is assigned a higher stage after resection. However, this change reflects more complete information rather than disease progression in the short time between procedures.
The tumor’s true extent was already present. It simply could not be fully assessed until the entire specimen was available for examination.
Conversely, some tumors suspected to be advanced based on imaging may turn out to be lower stage on final pathology. Both scenarios illustrate the importance of comprehensive surgical evaluation.
At Honest Pathology, we emphasize that staging evolves as more data becomes available. The biopsy is the first step, not the final word.
Does Understaging on Biopsy Affect Prognosis?
Prognosis depends on the final pathologic stage, not the preliminary biopsy findings. While initial expectations may shift, treatment planning is adjusted accordingly once definitive staging is known.
If lymph nodes are positive on resection, chemotherapy may be recommended even if the biopsy report did not suggest advanced disease. This is not a sign that something was missed earlier. It reflects the reality that biopsies cannot assess lymph nodes or full tumor depth.
Patients often search for reassurance that a change in stage means the cancer spread rapidly. In most cases, it did not spread between biopsy and surgery. The more complete examination simply revealed information that was not visible in the smaller sample.
Why Complete Pathology Review Matters
Colon cancer management depends heavily on precise pathologic evaluation. Accurate assessment of tumor depth, lymph node involvement, and margin status directly informs prognosis and therapy.
Pathologists play a central role in this process. Detailed sampling of the tumor, careful lymph node dissection, and thorough microscopic examination ensure that staging is as accurate as possible.
Understanding the limitations of biopsy helps set realistic expectations. A biopsy answers whether cancer is present. A resection determines how advanced it is.
The Takeaway on Colon Cancer Biopsy and Staging
Colon cancer can indeed be understaged on biopsy because a biopsy samples only a small, superficial portion of the tumor and does not include lymph nodes. Definitive staging requires examination of the full surgical resection specimen.
Differences between biopsy and resection reports are common and expected. The biopsy establishes the diagnosis. The resection provides complete staging information that guides treatment decisions.
If a stage changes after surgery, it reflects more comprehensive evaluation rather than sudden progression. Understanding this distinction can reduce confusion and help patients interpret their pathology reports with greater clarity.
Clear, accurate pathology reporting is essential to high-quality colon cancer care. When the differences between biopsy findings and final staging are explained thoughtfully, patients are better equipped to understand their diagnosis and move forward with confidence.