Inflammatory bowel disease affects millions of people worldwide, and the two main forms, Crohn’s disease and ulcerative colitis, often create confusion because they share many symptoms yet behave very differently in the body. Patients who receive a diagnosis or an inconclusive biopsy frequently search for straightforward answers about how the conditions differ clinically, what the pathology slides actually show, and whether one carries a higher long-term cancer risk than the other. Distinguishing between Crohn’s disease and ulcerative colitis is essential because treatment plans, surveillance strategies, and prognosis vary significantly. Pathology evaluation of colon or ileum biopsies plays a central role in making this distinction, revealing microscopic patterns that clinicians cannot see during endoscopy alone. Honest Pathology offers specialized pathology consultations that translate these detailed biopsy findings into clear, patient-friendly explanations, empowering individuals to understand their exact diagnosis and participate confidently in treatment decisions.
How Crohn’s Disease and Ulcerative Colitis Differ Clinically
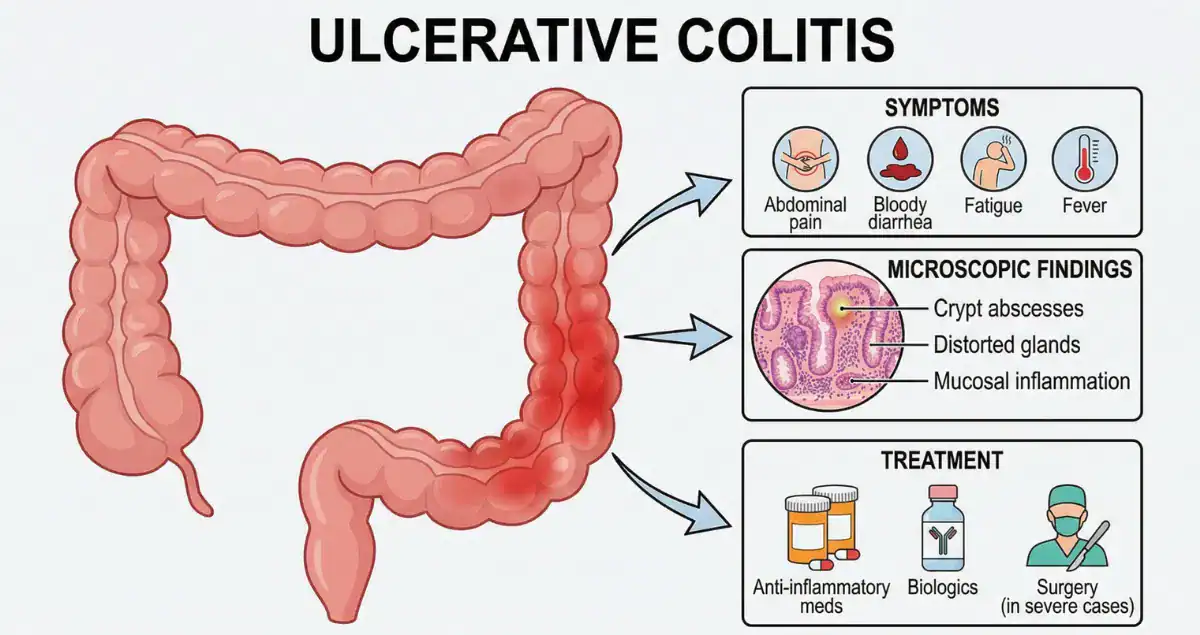
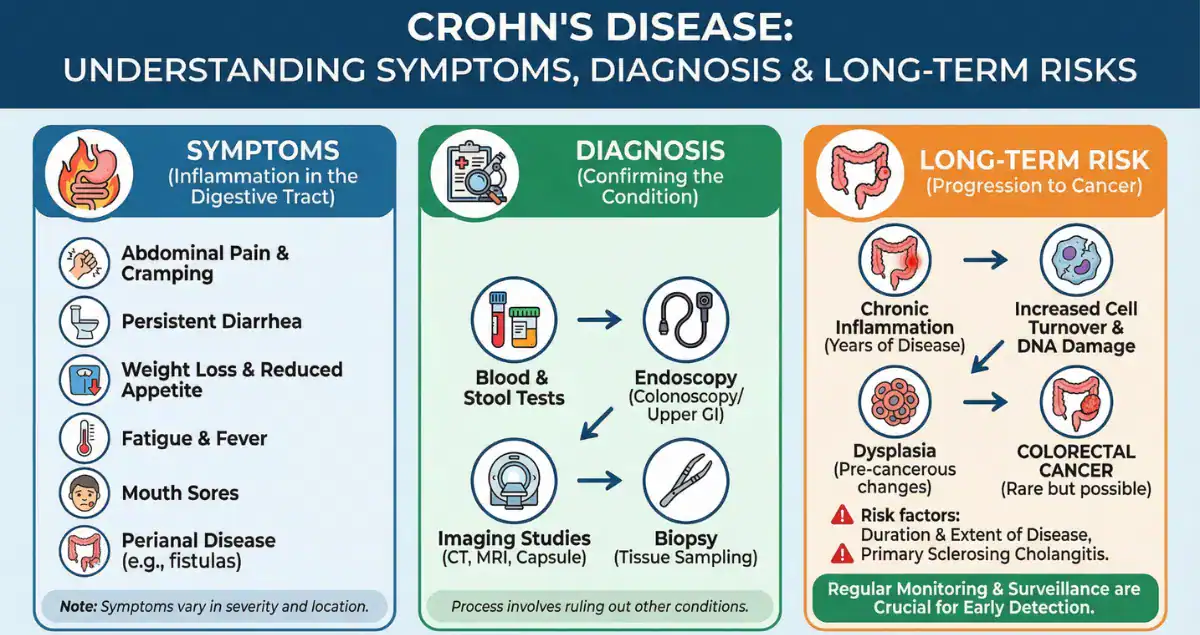
Crohn’s disease and ulcerative colitis both cause chronic inflammation of the gastrointestinal tract, but the location and depth of that inflammation create distinct clinical pictures. Ulcerative colitis is limited to the colon and rectum and almost always begins in the rectum, spreading continuously upward without skipping areas. Patients typically experience bloody diarrhea, urgency, frequent small bowel movements, and a sensation of incomplete evacuation known as tenesmus. Symptoms are usually confined to the large intestine, and complications such as toxic megacolon can occur in severe flares. In contrast, Crohn’s disease can affect any part of the digestive tract from the mouth to the anus, most commonly the terminal ileum and colon. It produces patchy, skip lesions with normal tissue in between. Diarrhea is often non-bloody or only intermittently bloody, and patients may also report abdominal pain, weight loss, fatigue, and perianal problems such as fistulas or abscesses. Because Crohn’s inflammation is transmural, penetrating all layers of the bowel wall, it can lead to strictures, fistulas, and abscesses that are rare in ulcerative colitis. These clinical differences guide initial management, yet biopsies are frequently needed when the pattern is not classic. Honest Pathology consultations help patients see how their symptoms align with the microscopic findings, clarifying why one diagnosis fits better than the other.
 Microscopic Differences on Biopsy: What Pathologists Look For
Microscopic Differences on Biopsy: What Pathologists Look For
The microscopic appearance on biopsy is often the most reliable way to separate Crohn’s disease from ulcerative colitis. In ulcerative colitis, inflammation is diffuse and continuous, limited mainly to the mucosa and submucosa. Pathologists observe uniform crypt distortion, basal plasmacytosis, and crypt abscesses throughout affected areas, with no skip lesions and no granulomas. The deeper layers of the bowel wall are spared. Crohn’s disease, however, shows patchy inflammation that can involve any layer of the bowel wall. Biopsies reveal focal crypt distortion, lymphoid aggregates, and, in about 30 percent of cases, non-caseating granulomas, small collections of immune cells that are highly suggestive of Crohn’s when present. Fissuring ulcers that extend deep into the wall are another hallmark of Crohn’s. Even when endoscopy looks similar, these histologic patterns allow pathologists to classify the disease accurately in most cases. Sometimes biopsies are inconclusive, especially early in the disease or after treatment has begun. Honest Pathology specializes in reviewing these slides in detail, explaining exactly which features support Crohn’s, ulcerative colitis, or an indeterminate colitis picture, so patients receive a precise explanation rather than vague terminology.
Shared and Distinct Complications Beyond the Intestine
Both conditions can cause systemic effects such as joint pain, skin rashes, eye inflammation, and bone loss, but certain complications are far more common in one than the other. Ulcerative colitis is associated with a higher risk of primary sclerosing cholangitis, a liver condition that itself increases colorectal cancer risk. Crohn’s disease more frequently leads to malnutrition, small-bowel bacterial overgrowth, and kidney stones due to its ability to affect the ileum. Perianal disease and fistulas are almost exclusive to Crohn’s. These differences influence not only daily symptoms but also long-term monitoring needs. Patients often wonder which condition is “worse,” yet both can range from mild to severe, and modern therapies have dramatically improved quality of life for both. Honest Pathology places biopsy results in this broader clinical context, helping patients understand why certain complications are more likely and what surveillance is recommended.
Cancer Risk in Ulcerative Colitis Versus Crohn’s Disease
Long-standing inflammation in either disease increases the risk of colorectal cancer, but the pattern and degree of risk differ. In ulcerative colitis, the 10-year cumulative risk of colorectal cancer is approximately 2 percent for patients with extensive disease, rising to 8 percent at 20 years and 18 percent at 30 years when the entire colon is involved. Risk is highest in those with primary sclerosing cholangitis or a family history of colorectal cancer. Because the inflammation is continuous and mucosal, surveillance colonoscopy with biopsies can detect dysplasia early. Crohn’s disease carries a similar overall colorectal cancer risk when the colon is extensively involved, though the 10-year risk is generally estimated at 1 to 3 percent in colonic Crohn’s. However, Crohn’s also raises the risk of small-bowel adenocarcinoma in areas of chronic ileal inflammation, a cancer that is extremely rare in ulcerative colitis. In both diseases, the greatest risk factor is the duration and extent of uncontrolled inflammation rather than the diagnosis itself. Successful maintenance therapy that keeps inflammation suppressed can substantially lower these risks. Patients frequently ask whether one condition is more dangerous from a cancer standpoint. The answer depends on disease extent and control: pancolitis ulcerative colitis and extensive colonic Crohn’s both warrant vigilant surveillance, usually beginning eight to ten years after diagnosis. Honest Pathology consultations identify any microscopic dysplasia or high-risk features on biopsy, giving patients a clear picture of their personal cancer risk and the rationale for recommended colonoscopy intervals.
Indeterminate Colitis: When Biopsies Do Not Clearly Separate the Two
In up to 10 percent of cases, biopsies show features of chronic colitis but lack definitive traits of either Crohn’s or ulcerative colitis. This situation is termed indeterminate colitis. Patients may have overlapping clinical and histologic findings, and the diagnosis can evolve over time as more information becomes available. Treatment often begins similarly for both diseases, with escalation based on response. Honest Pathology reviews these challenging cases thoroughly, noting which features lean toward one diagnosis over the other and explaining why a definitive label may not yet be possible. This clarity helps patients avoid unnecessary worry and focus on controlling inflammation while additional clinical data accumulate.
Common Questions Patients Ask About Crohn’s Disease and Ulcerative Colitis
Many individuals wonder whether it is possible to have features of both conditions at the same time. While true overlap is rare, indeterminate colitis exists precisely because the boundary is not always sharp. Another frequent concern is whether a diagnosis can change from ulcerative colitis to Crohn’s or vice versa after initial biopsies. Yes, this can happen in a small percentage of cases as the disease declares itself over time or after surgery. Patients also ask about the role of genetics and whether family history predicts one form over the other. Both diseases have genetic components, but they are not strictly inherited, and most patients have no affected relatives. Questions about cancer surveillance are common as well: guidelines recommend regular colonoscopy for both conditions once the disease has been present for eight to ten years, with more frequent exams if high-risk features are present on biopsy. Honest Pathology directly addresses these questions by reviewing the specific microscopic details in each patient’s report and placing them in the context of current clinical guidelines.
How Honest Pathology Empowers Patients Facing a New IBD Diagnosis
A pathology report describing chronic colitis, crypt distortion, granulomas, or indeterminate features can feel overwhelming and technical. Honest Pathology offers dedicated consultations that demystify every element of the biopsy: the pattern of inflammation, the presence or absence of granulomas, the degree of crypt distortion, and what these findings suggest about Crohn’s disease versus ulcerative colitis. Patients receive a clear, personalized explanation of their cancer risk based on the microscopic picture and learn exactly why certain surveillance or treatment recommendations are being made. This level of understanding allows more productive conversations with gastroenterologists and helps individuals feel in control rather than confused by medical jargon. Whether the diagnosis leans toward Crohn’s, ulcerative colitis, or remains indeterminate, Honest Pathology turns complex histology into practical knowledge that supports better long-term outcomes.
Crohn’s disease and ulcerative colitis share the common thread of chronic intestinal inflammation, yet their clinical behavior, microscopic patterns, and associated risks differ in important ways. Accurate differentiation through expert pathology review is the foundation for effective, personalized care. By providing clear explanations of biopsy findings, cancer risk estimates, and the rationale behind management plans, Honest Pathology empowers patients to move beyond uncertainty and take an active role in protecting their health. With modern therapies and regular surveillance guided by precise pathology insight, most individuals with either condition can achieve excellent quality of life and significantly reduced cancer risk.