Chronic inflammation on biopsies represents one of the most frequent yet confusing findings patients encounter after endoscopic or needle procedures. Whether the report mentions lymphocytes, plasma cells, or macrophages infiltrating tissue, many individuals immediately search online for answers about what it signifies for their gastrointestinal tract, breast, or lungs. This pattern differs sharply from acute inflammation, which features short-lived neutrophils rushing in to fight sudden injury. Chronic inflammation instead signals a prolonged immune response that can stem from ongoing irritation, infection, autoimmune activity, or environmental triggers. While it is rarely an immediate emergency, understanding its specific context in GI, breast, or lung biopsies can ease anxiety and guide next steps. Honest Pathology delivers clear pathology consultations that translate these technical reports into plain language, helping patients grasp their exact situation and become confident partners in their health decisions.
What Does Chronic Inflammation on a Biopsy Actually Mean?
Pathologists identify chronic inflammation by the types of immune cells present under the microscope and by the tissue changes that accompany them. Lymphocytes and plasma cells dominate the picture, often joined by macrophages that clean up debris over weeks or months. Fibrosis or scarring may appear as the body attempts repair, and the architecture of the tissue can become altered. Unlike cancer, this finding usually points to a reactive process rather than uncontrolled cell growth, although longstanding inflammation occasionally raises the risk of certain complications or even malignancy in susceptible organs. Patients commonly wonder whether the biopsy itself caused the inflammation; in reality, the procedure may produce localized reactive changes, but true chronic inflammation reflects conditions that existed before the sample was taken. Accurate interpretation hinges on clinical context, imaging, and sometimes special stains or molecular tests, which is precisely why expert pathology consultation proves essential for turning raw data into actionable understanding.
Chronic Inflammation in Gastrointestinal Biopsies: Esophagus, Stomach, and Colon Insights
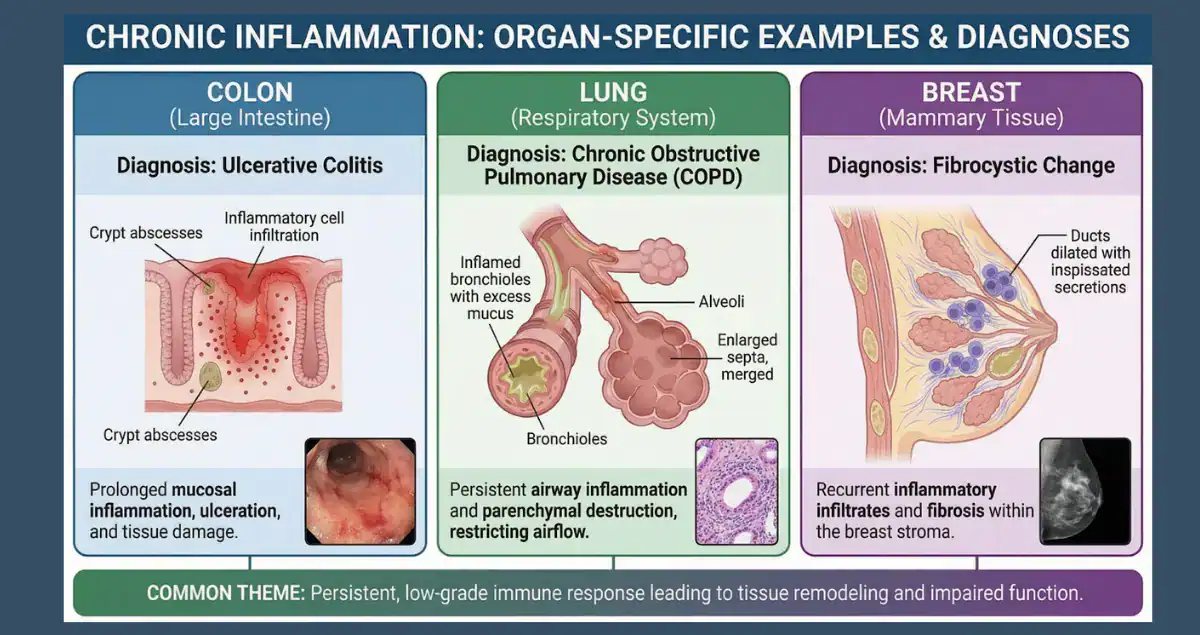
Gastrointestinal biopsies frequently reveal chronic inflammation because the digestive tract constantly interacts with food, bacteria, acid, and medications. In esophageal samples, chronic esophagitis most often arises from gastroesophageal reflux disease, where repeated exposure to stomach acid damages the lining. Patients may experience heartburn or swallowing difficulty, and the biopsy shows basal cell hyperplasia along with intraepithelial lymphocytes. When inflammation persists at the gastroesophageal junction, known as carditis, it can link to either Helicobacter pylori infection or reflux, sometimes progressing toward intestinal metaplasia that warrants surveillance. Stomach biopsies commonly demonstrate chronic gastritis, with H. pylori as the leading culprit worldwide. The organism triggers a persistent lymphocytic infiltrate that may thin the mucosal lining over time, raising the risk of ulcers or, in rare cases, gastric cancer if atrophy and metaplasia develop. Autoimmune gastritis presents a different pattern, targeting acid-producing cells and often associating with vitamin B12 deficiency. Moving to the small intestine and colon, chronic inflammation frequently signals inflammatory bowel disease.
Duodenal biopsies in suspected celiac disease display increased intraepithelial lymphocytes and villous blunting, while colonic samples from ulcerative colitis or Crohn’s disease feature crypt architectural distortion, basal plasmacytosis, and patchy or continuous involvement depending on the subtype. Microscopic colitis, another common cause, produces watery diarrhea despite endoscopically normal-appearing mucosa, yet biopsies uncover dense lymphocytic or collagenous bands beneath the surface. Patients searching “chronic inflammation GI biopsy meaning” often ask whether this automatically means inflammatory bowel disease or cancer. The answer depends on the exact location, pattern, and additional features; many cases remain benign and respond to lifestyle adjustments, acid suppression, antibiotics, or anti-inflammatory medications. Pathology consultation clarifies these distinctions so patients can discuss targeted therapies with their gastroenterologist rather than guessing from general online information.
Chronic Inflammation in Breast Biopsies: Patterns, Causes, and Patient Concerns
Breast biopsies showing chronic inflammation typically arise in benign conditions, though the finding still prompts questions about cancer risk. Common scenarios include periductal mastitis, where lymphocytes and plasma cells surround dilated ducts, often in smokers or women with nipple discharge. Fat necrosis after trauma or surgery produces foamy macrophages and chronic inflammatory cells amid scarred tissue, mimicking a mass on imaging. Granulomatous lobular mastitis stands out as a distinct entity with clusters of macrophages forming granulomas, frequently linked to autoimmune processes or prior infections, and it can cause painful lumps that recur without proper management. Post-biopsy changes themselves sometimes contribute localized chronic inflammation, with macrophages lingering around needle tracts for weeks or months, accompanied by foreign-body reactions if clips or markers remain. Patients frequently worry whether chronic inflammation on breast biopsy increases the chance of developing breast cancer later.
Research suggests that certain inflammatory patterns in benign tissue may correlate with modestly elevated risk in some populations, particularly when dense breasts or obesity coexist, yet the vast majority of isolated chronic inflammation remains non-malignant. Treatment varies widely: antibiotics or steroids for granulomatous cases, observation for mild reactive changes, or further imaging if the inflammation obscures underlying lesions. Because breast biopsies balance cancer exclusion with benign explanations, an expert pathology consultation helps patients understand whether their report shows simple reactive inflammation, a specific inflammatory disorder, or features that merit closer follow-up, empowering them to ask informed questions during surgical or oncology visits.
Chronic Inflammation in Lung Biopsies: Interstitial Lung Disease and Beyond
Lung biopsies revealing chronic inflammation often fall under the broad umbrella of interstitial lung disease, where persistent immune activity damages the delicate air sacs and supporting framework. Patterns vary: usual interstitial pneumonia, the hallmark of idiopathic pulmonary fibrosis, features patchy fibrosis with fibroblast foci and relatively mild lymphocytic inflammation, predominantly in the lung periphery. Nonspecific interstitial pneumonia displays more uniform cellular infiltrates of lymphocytes and plasma cells throughout the alveolar walls, sometimes linked to connective-tissue diseases like rheumatoid arthritis or scleroderma. Hypersensitivity pneumonitis introduces poorly formed granulomas amid centrilobular inflammation, triggered by repeated inhalation of organic dusts, molds, or bird proteins. Sarcoidosis produces well-formed non-necrotizing granulomas that can cluster in lymph nodes and lung parenchyma, while organizing pneumonia shows plugs of fibroblasts within small airways surrounded by chronic inflammatory cells.
Patients searching “chronic inflammation lung biopsy” commonly ask about progression to scarring or breathing decline. Many forms of interstitial lung disease do involve fibrosis that stiffens the lungs over time, reducing oxygen transfer, yet early identification of the precise pattern allows interventions such as antifibrotic medications, immunosuppressants, or removal of environmental triggers to slow or stabilize disease. Smoking, occupational exposures, or autoimmune conditions frequently underlie these changes, and accurate subtyping through biopsy guides prognosis discussions. Here again, specialized pathology review integrates histologic details with clinical history to differentiate idiopathic processes from treatable secondary causes, giving patients the clarity needed to pursue pulmonary rehabilitation, oxygen therapy, or clinical trials when appropriate.
Answering the Most Common Questions About Chronic Inflammation on Biopsies
Patients across GI, breast, and lung biopsy results share several recurring concerns. The top question remains whether chronic inflammation equals cancer; in the overwhelming majority of cases the answer is no, although certain chronic patterns can raise long-term risk in the esophagus, stomach, or breast tissue and therefore require monitoring. Another frequent inquiry addresses causes: possibilities range from infections like H. pylori, reflux, or environmental allergens to autoimmune disorders and even the body’s reaction to prior injury or foreign material. Treatment questions follow naturally, what can be done? Options depend entirely on the site and trigger. Proton-pump inhibitors heal esophageal inflammation, eradication therapy clears gastric H. pylori, dietary gluten avoidance reverses celiac changes, and anti-inflammatory or biologic drugs manage inflammatory bowel disease. Breast cases may need steroids or surgical drainage for granulomatous mastitis, while lung inflammation often responds to corticosteroids, antifibrotics, or allergen avoidance.
Prognosis varies just as widely; mild esophageal or gastric inflammation frequently resolves completely, whereas progressive interstitial lung disease may require lifelong management yet still allow good quality of life with early intervention. Follow-up timing also generates searches: some patients need repeat endoscopy or imaging in months, others annual surveillance, and many simply benefit from symptom tracking. Finally, individuals ask whether genetic testing or lifestyle changes matter. In select GI and lung scenarios, inherited predispositions or modifiable factors such as smoking cessation and weight management can influence outcomes dramatically. Honest Pathology’s consultations address all these questions by breaking down the report line by line, explaining why certain cells appear, what they imply for each organ, and which details deserve immediate attention versus routine observation.
How Pathology Consultations Empower Patients Facing Chronic Inflammation Findings
Receiving a pathology report that highlights chronic inflammation can feel isolating when medical terminology overshadows practical meaning. Honest Pathology specializes in patient-focused pathology consultations that bridge this gap. Rather than leaving individuals to decipher dense descriptions alone, these reviews provide straightforward explanations tailored to the biopsy site, whether gastrointestinal, breast, or lung, while highlighting any molecular or special-stain results that refine the diagnosis. Patients leave the conversation equipped to discuss specific therapies, surveillance intervals, or lifestyle adjustments with their treating physicians. In an era when online searches yield conflicting generalities, personalized pathology insight transforms uncertainty into empowerment. Individuals gain the confidence to request second-level testing if needed, advocate for multidisciplinary input, and focus on what truly matters: addressing the root cause and protecting long-term health.
Chronic inflammation on biopsies, whether discovered in the esophagus, stomach, colon, breast ducts, or lung interstitium, reflects the body’s sustained response to persistent challenge. Far from a uniform diagnosis, it encompasses dozens of distinct patterns, each carrying unique implications and management strategies. By seeking expert pathology consultations early, patients move beyond fear of the unknown and step into informed participation in their care. Honest Pathology stands ready to deliver that clarity, ensuring every individual understands their report in depth and feels prepared to navigate the path ahead with knowledge, partnership, and hope.